Pathology, at least when I first heard about it, seemed like the most boring field of medicine. Not boring in the sense that the subject itselssf is boring, such as how some topics in neuroscience are so confusing that it becomes mind-numbingly boring. Yet, when I heard about pathology, I thought it was boring in the sense that nobody really cares. From the mild research that I have done, they’re not quite recognized or mentioned at all when patients are treated and they have quite a relatively low salary as opposed to other specialties, yet it suddenly clicked. It is easily one of the most respectable medicinal fields, such as how a scriptwriter ties up a movie together.
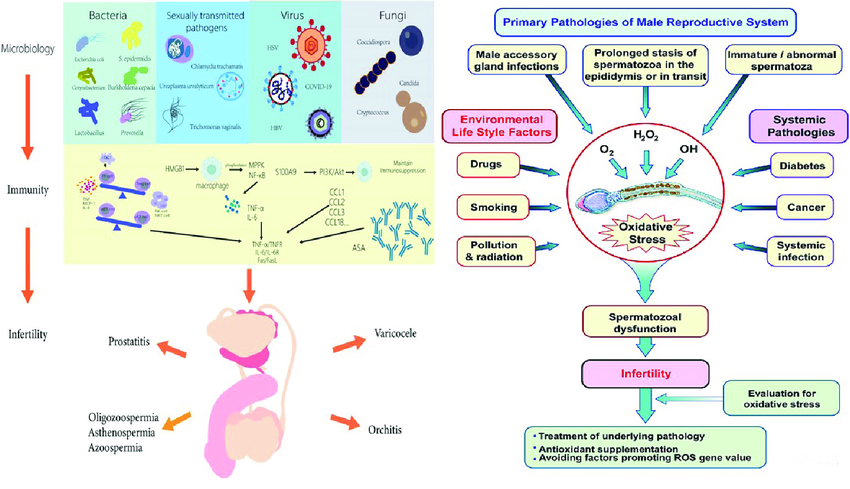
In essence, pathology is the study of the diseases, meaning the hours upon hours of biology revision can actually be effective in this field, as it focuses upon lower ranking doctors who study the diseases that are found in patients. Pathologists analyze diseases using four core steps, the etiology of the disorder, the pathogenesis of it, and the functional derangements and morphologic changes. The example shown below is a more detailed pathology of the male reproductive system.
The epitology is the cause of the disease, which is surpriingly difficult tp find out. An example could be the epitology of a male patient classed infertile. While it could just be a genetics or epigenetic issue, it could also be due to an excessive addiction to substances such as alcohol or nicotine (classified as endangering lifestyle factors). The way pathologists effectively identify the cause of said disease is using their clinical data with more advanced laboratory testing, using a systematic process called clinicopathologic correlation, matching the physical symptoms of their patient’s physical symptoms with their molecular and structural findings. In some cases where the disease is on a molecular, DNA level they use molecular testing, which allows them to identify the forefront fingerprints of the disease.
The pathogenesis is the sequence of events and biochemical changes that occur from a diseases first stage to it’s final one. The initial stage is the exposure, where the disease arrives at an opening such as a mouth or a wound, and it sticks to the cells using it’s own special structures so it sticks, not to be dragged away by the body’s natural cleansers (i.e; tears, excretion, urination). From now on it breaks through the inital barrier and enters the deeper tissues. From now on the disease/pathogen will replicate rapidly and secrete toxins that destroy the tissue directly.
Now morphologic changes are the changes that pathologists are actually able to see, meaning the physical changes seen in cells and organs (physical alterations to shape and size[yet these ‘physical changes’ are actually seen under a microscopic lens]). On the other hand, functional derangements are how the body behaves incorrectly or not normally due to those physical changes. Essentially the loss of basic, normal human function. The main symptoms of functional derangements are usually that the patient will naturally feel short of breath, tired and the heart mispumping (extremely irregular for even patientd with massive disorders). On an organ level, if the heart muscle suffers from morphologic change it will directly lead to heart failure (and this sort of change can also occur in other major organs).
While I still think pathologists aren’t recognized enough and that it’s quite a challenging subject, it’s still an absolutely fascinating, undervalued and lovely profession.
In all honesty, Neurology was not a field I had so much knowledge in compared to other fields, such as pediatrics or even physiotherapy. Sure, I had participated in that epilepsy awareness event, but my knowledge was just minimal. I mean, sure I was relatively familiar with mental disorders and whatnot, but having enough knowledge to write a whole research paper? Yeah right….Well, it’s been over three months since the awareness event, and I am glad to say what I had previously thought near-impossible, I have relatively completed.
The thing is, Neurology is such a complex subject with so many sub-branches and other topics, it’s near impossible to know every single thing about the brain, yet alone contain all of it into a single research paper. The brain is such a diverse area to study, so the main subjects I wanted to put into this paper are
Disorders
Aging
Social/Emotional Aspects of The Brain
But to state something before I start; I am not the Brad Pitt of neuroscience whatsoever. Even all this knowledge I am boasting about is quite minimal to what actual neurologists have to learn to actually become a neurologist. Yet, neurology is such a fascinating subject, there is always more to learn as the brain evolves and grows. Without futher ado, let’s start this.
Mental Disorders
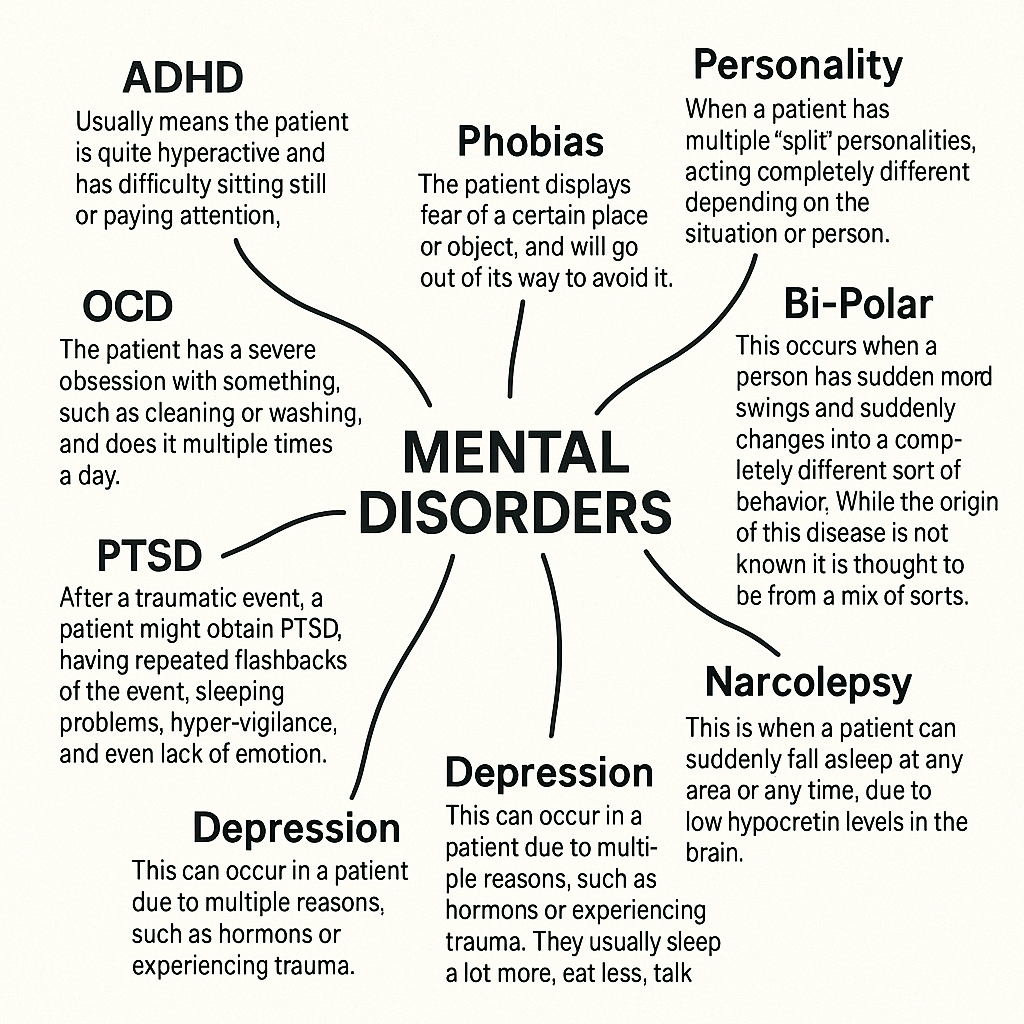
In the brain, there are certain parts of it assigned to certain areas of our life, such as thought, speech or comprehension. When these parts get damaged, whether that be through self-infliction or car accidents, they can lead to brain damage or impairment, which can lead to disorders. Most mental disorders are relatively harmless, such as attention-deficit-hyperactive-disorder (ADHD), not being able to sit still while watching a documentary, or obsessive-compulsive-disorder (OCD), having an obsession with cleaning your glass-model cars. Yet, some can end lives or indirectly cause massive bouts of harmsl such as schizophrenia, alzeihmers, or shock paralysis (yes, it sounds exactly like it’s spelled.)
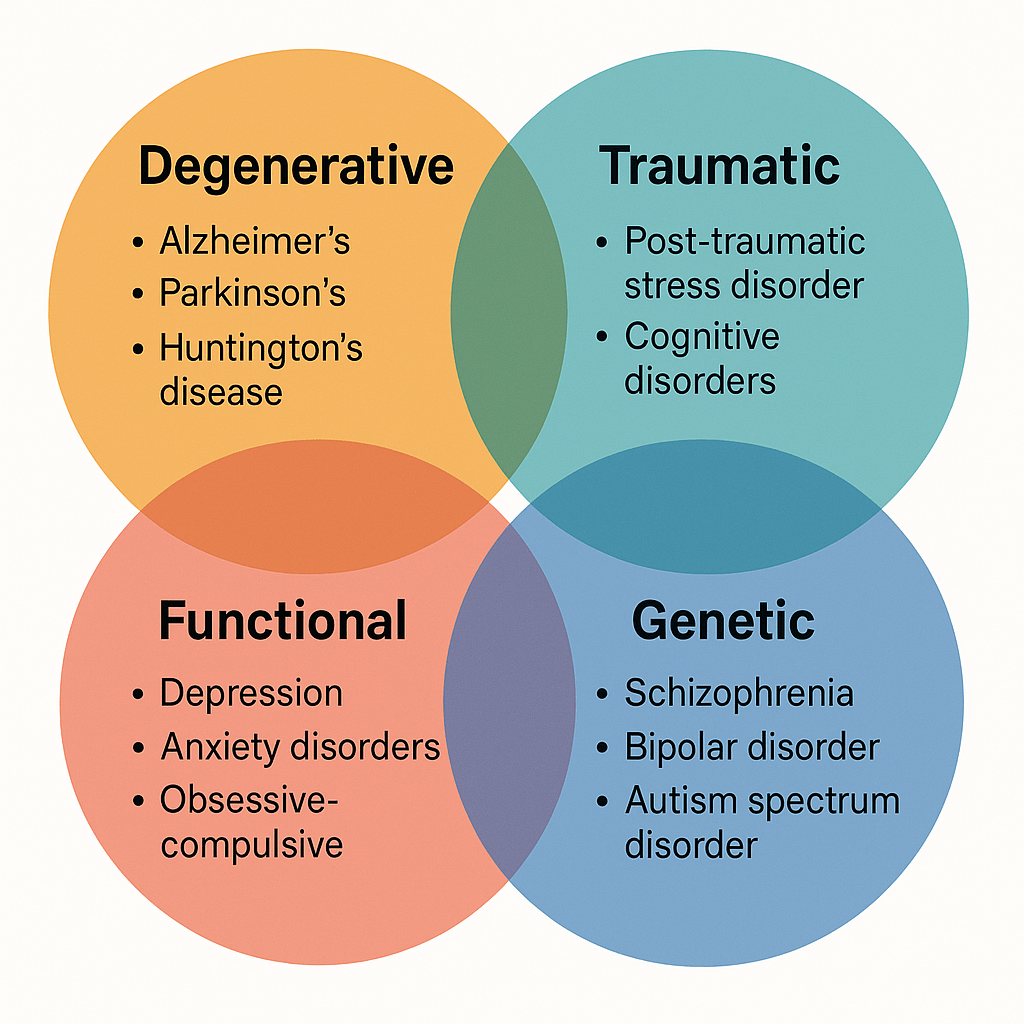
Yet, there are more reasons for disorders, and the most common of them are
Degenerative; These are mostly in older people. They are due to inactivity of their brain or muscles, making them more prone to crippling and making them weaker as a whole. These mental malfunctions can unfortunately accompany them, such as Alzheimer’s, tending to forget things as mild as grocery shopping to as severe as their own name. While contradicting my previous statement, not all of these disorders are technically ‘deadly’, yet they increase the risk of the elderly person too commit dangerous acts such as self-harm or reckless driving. These diseases are mostly present in elderly people over the age of 70, yet it’s not exactly uncommon for them to be within the range of 50-69.
Genetic; While the most common mental disorders are due to other factors, there are multiple disorders that can be contracted due to genes and genetics. These disorders are mostly uncontractable, yet there are other ways that they can be contracted other than genetics. Yet, just due to the fact that one family member had the disease does not mean that you will surely get it, as it can just be a one-time thing. These genes are mostly common in men (86%), yet some women also contract it.
Traumatic; These sort of disorders are quite common, and caused by experiencing traumatic events. These events can range from car accidents to war-time. Now, just experiencing these events does not directly mean that the patient will contract this disorder, yet it’s quite common to contract these disorders after these experiences. The most common disorder out of this type is post-traumatic-stress-disorder (PTSD), which have the symptoms of habing repeated lucid dreams about the events, and not being able to function properly, and mostly only being able to speak about the event.
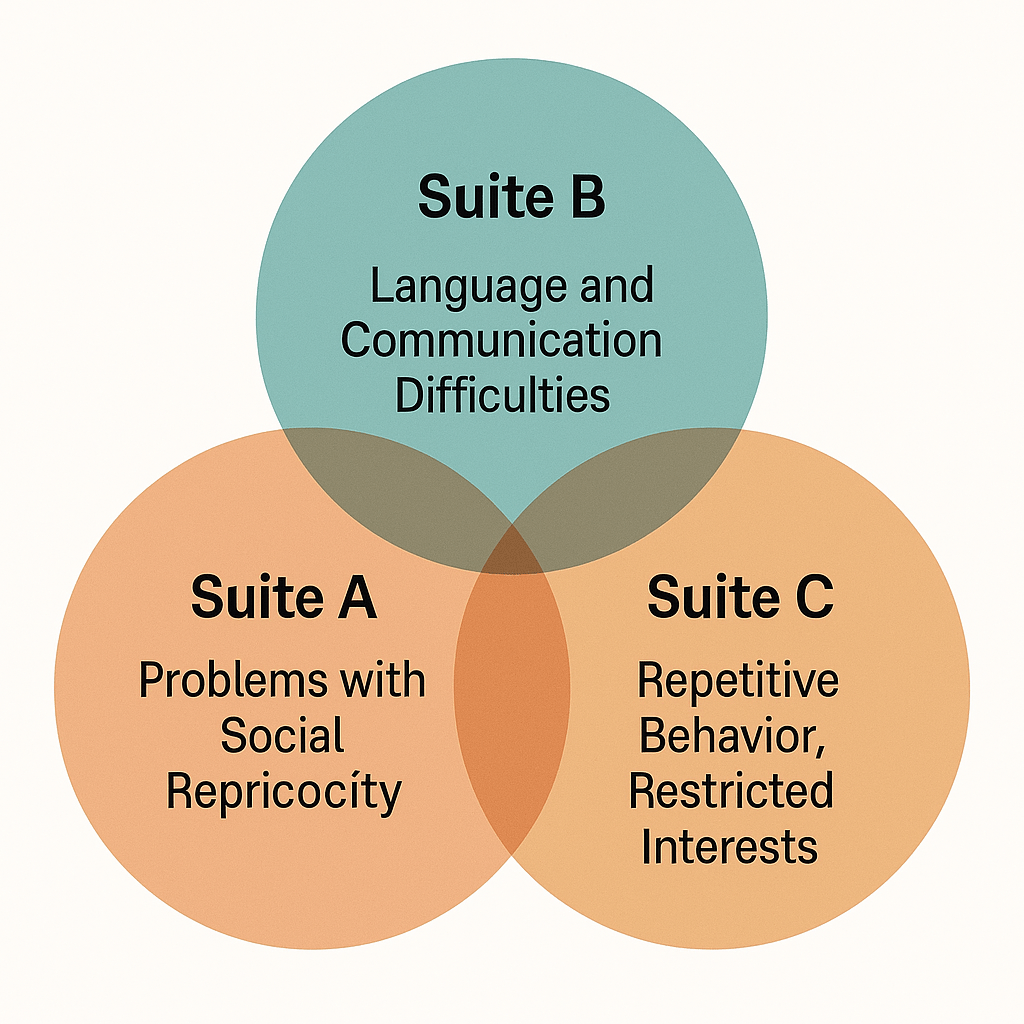
Now, there are multiple disorders that can be diagnosed on a spectrum, noticabely autism. Some people without autism show different forms/suites of behaviour, and the common behaviour in all suites lead to being diagnosed with autism. The common suites are presented in the diagram below.
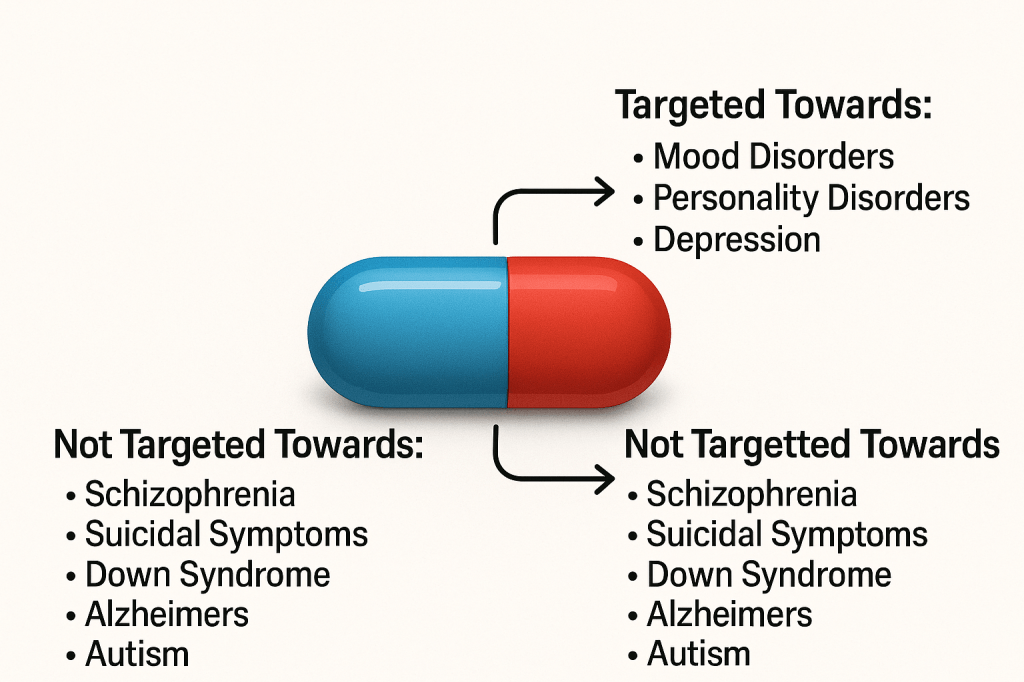
Evidently, there are treatments to these diseases, yet it’s not proven they have a perfect success rate. They mostly have quite a number of side effects, commonly being very emotional, tired or feeling very nauseous some time after taking the medication. Yet, this does not mean these meds are never presicribed, it’s quite the opposite. They are prescribed quite often, especially in anxiety disorders, or depression. They are never a permanent cure though, they are always part of a larger treatment plan to help ‘cure’ the disorder.
The most common medication type used are pills. While they are commonly used in the disorders explained above, they can also be used in ADHD or OCD, yet not as often. They help and calm the patients, and help deactivate the depressive hormones and increase dopamine, the hormone that makes you feel optimistic. These medications help regulate brain chemistry and reduce depressing/distressive symptoms in the patients, and overall help them function normally, though these medication obviously will not work for all disorders.
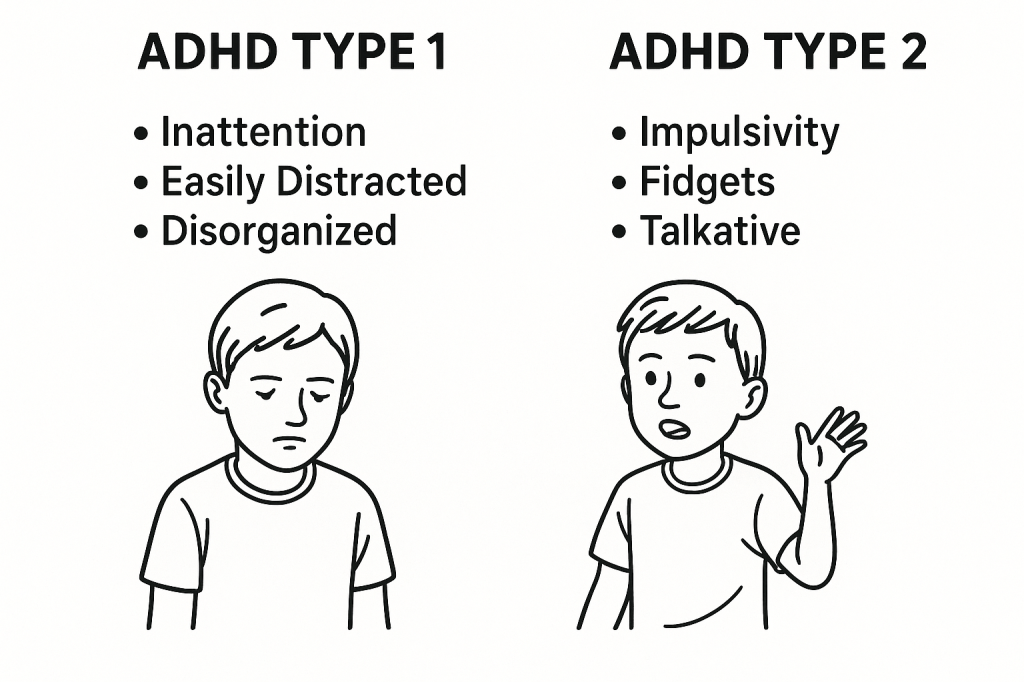
Now, the diagnostic aspects of the brain. Mental disorders as a whole cannot be identified just from a few symptoms; they have to genuinely interrupt everyday activities, such as school or dinner, and contain most symptoms to be properly identified. Usually, some physical tests by doctors are used to identify these disorders, yet multiple certified online tests can be used, though they could be inaccurate, or the patient self-diagnosing themselves. Though, eve after online diagnosation, it is evidently best to consult a local psychatrist or doctor. Adding to the symptoms aspect, not all symptoms have to be present. In ADHD, only a few symptoms are ‘compulsory’, such as inability to stop fidgeting, to be diagnosed with a certain ADHD type.
Yet, with more complicated diseases centered towards the brain sucb as epilepsy or schizophrenia, brain imaging scans are often used, such as CT scans and MRI’s.
In medieval days, mental illnesses are commonly regarded as the disease of the inner spirit during the middle ages. It was assumed that devils, or ‘foul spirits’, would enter a persons body, and make them ‘insane.’ The physical theories of mental illness were;
Imbalance of the four humors (which back then determined a persons health and wellbeing)
Blockage of multiple supernatural, healthy ‘forces’ and spirits, thought to be because the patient was a witch or some sort of demon
It was really in the nineteenth century, when the acclaimed Sigmund Freud thought up the idea of a subconcious. He developed the foundation of psychoanalysis, the idea of bringing hidden ideas to the consciousness, and the building block of therapy nowadays. The most common (and highly ineffective) treatment back then was hypnosis, and it was due to the invention of brain-scanning devices that proper treatment for disorders started to be used.
A reason why diagnosting is so important nowdays is the way it impacts indivuals, such as in acts of law. In severe cases of sexual assualt or murder, these alleged ‘criminals’, can technically have no charges pressed against them is if they are mentally damaged, or pleaded insanity. This can also decide upon multiple other important factors, suchh as whether they are suitable for certain types of employments (would someone with severe alzeihmers be quite suitable for customer service), or even eligible for government (or state aid).
Surpisingly, mental illnesses can also affect aging, especially in younh children, pre-puberty/adolescent. The way it impacts is by making the body phsyically incapable, passing aging checkpoints (i.e first steps, first words, jumping) way after it ideally should have done. Around 34% of autists are shorter than average and with less than 7% being taller than average.
}”
Now, I personally think I am finished with this topic, so it’s about time we move on.
Development and Aging
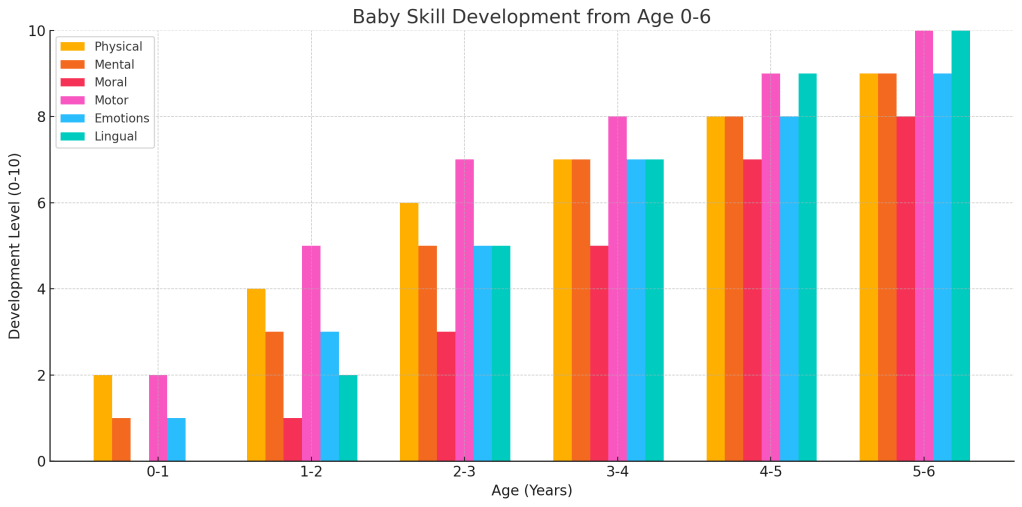
The human brain and body evolves and grows slightly differently deending on the person, but the brain development always stays the same. While the embryo is in the uterus, it slowly starts to develop its brain, starting with the neural tube, and slowly forming other parts such as the brain stem, cerebellum and cerebrum, with the sensory nerves also starting to develop. Finally, during birth, the baby develops nearly all 100 billion neurons, the same as an adult, yet nearly all of them are not mature, and develop until around the age of eighteen. The baby obviously starts to grow, and understand topics, developing multiple of the neurons, maturing quite rapidly. Yet speech, and a lot of similar characteristics are automatically wired into the brain, yet evidently all babies require appropriate simulation to actually develop the characteristics.
Now, the next step of growth is childhood to adolescence, where children develop motor skills and much more concepts that are extremely important during these years.
Yet during childhood (five to eleven years of age), there is not much significant development in the brain, except for noticable skill development and maturing through childhood experience, yet it’s really during the teenage/adolescent years that the body significantly changes like it had done during infantry.
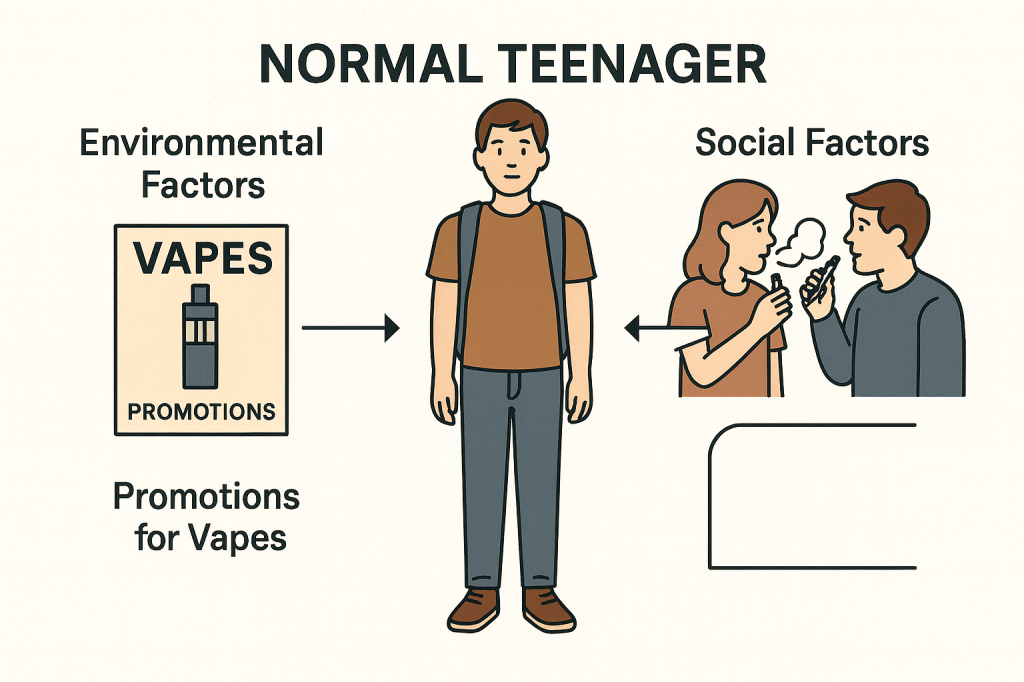
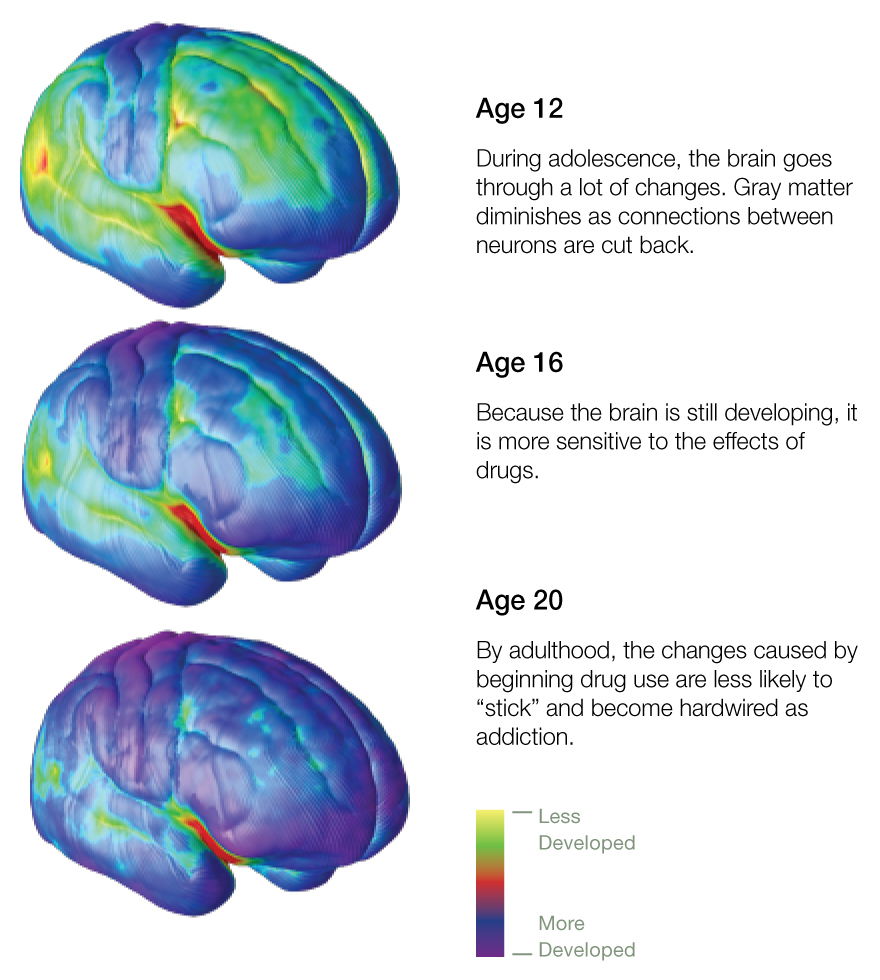
Between puberty and early adulthood, the human being goes through a renaissance-like stage. This process is well reflected in impulsive and rebellious behaviour, and eerily sudden personality changes. While all these changes take place, the teenage brain is quite vulnerable, and personality traits like risk-taking may be amplified to the extent that they can cause serious dysfuncton such as addictive drug-taking, criminal-like behaviour, and intense anxiety or depression. Fortunately, in many cases, the issue passes as the brain matures, yet it can sometimes signal the unofrutante start of long-term mental health problems, that can last even throughout adulthood. These changes in the teenage brain (in both genders) are driven by testosterone release, and the hormones make neural pathways extremely flexibile, in the sense that connections can make or break quite easily. On the positive, this allows teenagers to learn new things quickly, and to adapt to new habits and personality traits. Yet, on the negative side, this can lead to easily being influenced, and being more inclined to risk-taking, rebellious and somewhat pessimistic behaviour, which can lead to self-inflicted trauma, in severe cases.
Their pre-frontal cortex is still developing, which is thought to be one reason for teenagers to be more inclined to this sort of behaviour, yet it’s obvious this behaviour can be present due to an addition of enviromental and social factors. The pre-frontal cortex is closely connected to the basal-ganglia which plays a quite important role in the development of motor skills. The fibre that links the two hemispheres in the brain-the corpus collosum-thickens, allowing for increased information to information processing skills.
During the teenage years, the patients have a high risk of being diagnosed with a mental illness, commonly ADHD and Anxiety, yet when teenagers experience traumatic events, they are extremely likely to contract a severe disease such as PTSD or Schizophrenia. When these patients near early adulthood, they are likely to contract a substance addiction, commonly alchohol, drugs, or cigarretes.
Most teenagers (commonly women), tend to get quite emotional very easily, thought to be due to the limbic system in the brain, which helps control our emotions. During puberty, the system is surprisingly active compared to any other time period, and this leads to the emotions being extremely prominent, and outbursts of sudden rage, or sadness occuring quite often, During early adulthood, the system matures, helping handle emotions significantly better.
Now during adulthood, the brain doesn’t stop growing. Like any other organ, the brain continues to reform itself long into adulthood. New brain cells continue to be created, and the architecture of the brain is changed constantly in response to life experiences. Humans brains are, compared to most animals, are quite slow to reach adulthood. The prefrontl cortex is the last part to actually become fully active, and full myelination-the sheathing of neuronal connections, which allows information to flow freely along them-does not occur until late into their twenties or thirties. Once the pre-frontal cortex is fully online, it becomes more active in situations that require emotional contenrl Whereas a teenage, or even a child might be overwhelmed by emotion, the prefrontal cortex inhibits emotion when necessary, and so allows for a more thoughtful, deliberated response.
Now, with the creation of new brain cells allow new information to be stored, but their arrival disrupts exisiting memories form in the hippocampus and are tranferred to long term storage in other brain areas. For a while, the memory resides both in the hippocampus and elsewhere. After a few years, the memory is cleared from the hippocampus. Until the memory is fully transferred, the arrival of new cells in the hippocampus may weaken the connections encoding memories stored there.
It is thought that the number of brain cells in the adult brain was fixed early in life and that laying down new memories and learning new things was achieved entirely by changes to existing neurons and their connections with one another. While this sort of rewiring is important for learning, it is now known that adults also benefit from the creation of new brain cells. Neurogenesis, the name for it, occurs mainly in the denate gyrus of the hippocampus. About a third of the neurons in the adult hippocampus are replaced in a person’s lifetime. Adding to this, a person’s brain continues to mature until their late twenties. The main changes take place inside the higher functional areas of the brain, such as the frontal cortex, which gradually becomes more active-pulling together information from the rest of the brain and forming a complex and holistic view of the world. Until then, the emotional parts of the brain are not fully connected with those areas concerned with thought, judgement, and behavioural inhibition. As the connections between the areas become more stable, people tend to react less emotionally and impulsively-instead becoming more cautious, considered, and exercising better judgement.
Now, onto the ageing brain. See, the traditional normalized view (probably thanks to the completely medical accurate ‘Simpsons’) is that the brain and body start to sort of degenerate. This is relatively true, but in the fact that neurons are ..’lost’, and for those that remain, impulses are transmitted much slower than normal. This obviously leads to slowing thought processes, memory problems, and deteriorating reflexes, which causes problems with physical aspects of the body, such as balance and movement.
In the past (meaning ‘cursive handwriting’ level old), it was quite rare for people to live above the age of 50, so we have not evolved much to use the brain in such advanced years. This makes the ageing brain quite a relatively new phenomenom. The degeneration of the brain and nervous system is not caused by a diseasee, and so should not be confused with the pathology of dementia, (which, in fact, is associated with patterns in specific brain changes). Now, recent research shows that most neurons actually remain healthy until you die, but the heart volume and size decrease around 6-10% from the age of 20-90.
One weird thing is that age can affect excitement levels (not in the way you think of, where old people sit around gossiping and yelling at children riding bicycles), but in a scientific kind of way. Dopamine, the neurotransmitter that triggers excitement, rapid decisions and overall happiness. Brain-imaging studdies show that as people age, their dopamine circuits decrease. This is associated in behavioral changes, as dopamine is associated with thrill-seeking and risk-taking. Neurologists believe it is due to the fact that older people seek a quieter life, or even a less thrill life as their dopamine is less abundant. An example could be any holiday where you recieve presents, such as Christmas. Opening presents is highly exciting for childrens and adolescents, but evidently much less so for adults and the elderly, as dopamine is triggered by rewards, or gifts, which also has much less impact as you age.
Now, ageing is not all pessimistic as I had explained before, and there are also positive aspects. The brain can compensate for the effects of ageing, and mental function can even improve with age. Myelin increases in the temporal and frontal lobes in the 45-50 age group could enable people to manage their knowledge better. Not only that, comprehension studies have shown that high-functioning elder adults use both brain hemispheres, which is sort of the brain’s memory to keep thought and memory processes stronger, an apology for making most of the body quite declining and useless.
Now, even newer research into ageing shows that the rate if decline could be slowed by positive lifestyle factors, such as regular exercise. Research has also found that reducing food intake, resulting in lower blood glucose levels, may slow the pace of change, as blood glucose can cause damage to enhancing proteins. Certainly, people with elevated blood glucose lvels, such as those with T.1 diabetes show more signs of brain ageing than non-diabetic people. There are evidently multiple benefits of a healthy lifestyle, such as simulating neural tissue growth. Gentle aerobic exercise, such as rapid walking, regular sleep, a healthy and balanced diet are expected to help delay age-related mental issues such as memory loss.
Now, while the next few paragraphs of this next topic are not exactly connected to the ageing of brains, but rather the ‘Brain of the Future’. While it sounds extremely cliché, the fantasty that has existed since 1984 with The Terminator is now extremely close to being real. As we discover how the brain works, the prospect of changing it, enhancing it, and developing artificial brains is quickly becoming fact rather than fiction, as stated before. Technologies for mind reading, thought control, and AI machines are already with us, and are becoming more sophiscated every day.
When a person is thinking, their brain produces mild electric signals. Neuroscientists have discovered ways in which the eletric signals are able to be picked up by sensors and sent wirelessly and sent to other electrical devices, making it quite possible to move or alter objects by literally pure thought. Most research in this field is directed towards developing devices that are able to help people with nervous-system injuries regain the use of limbs previously paralysed. The technology has also been picked up by multiple game factories, who have produced games that can be played using thought power.
To add to what explained previously on mind reading, the way it’s made is through the neural activity. The ‘picture’ of neural activity created by fMRI scanning can be sort of translated into a accurate description to what a person is seeing and thinking (to some extent). The way this is formed is that the output of the scan, captured while they are looking at a particular image, is processed by sophiscated computer software that translates the pattern of activity into a sort of ‘read aloud’. Such ”mind reading” is made possible as neurons in the visual cortex are specialized for specific stimulti–horizontal/vertical lines, so their firing patterns are indicative of the tyoe of visual stimuli the neurons are registiring. This also helps with lie detection. Now, finally onto the next topic.
The Social & Emotional Aspects
Emotions are generated in the limbic system, explained before as used a lot in adolescents to generate emotionally type responses. Each emotion is produced by a different ‘network’ of brain modules, including the hypothalamus and pituitary gland; which control the hormones that produce physical reactions such as increased heart rate and muscle contraction.
Now, we have evolved a ‘conscious’ emotional system, yet we still retain the primitive, automatic responses at the heart of emotion. An example could be hearing a frightening sound, we register it into the amygdala before we are even conscious of it. While the sensory information is sent to the cortex to be made conscious, the amyglada sends messages to the hypothalamus, which trigger changes that ready the body for fligh, fight, or appeasement. This quick route allows us to take instant action to save ourselves. When we ‘start’ at a loud sound, then relax on realizing that it is harmless. we are experiencing both stages-conscious and unconscious responses and reactions.
When it comes to social and emotional aspects, emotions in nearly everyone are quite conscious, and we’re usually aware of what emotions we’re feeling at every moment, but they’re not something physical, just our brain’s natural response to stimuli, designed to push us away from danger and towards reward or comfort, hence the term comfort zone. Emotions are generated quite constantly, yet there are so much we’re only aware of the predominant ones. (When I say ‘natural response’, while I do mean what our brain’s naturally designed to, but the brain as said before is also affected by environmental factors. Meaning if someone grew up in an area where danger was quite normal and encouraged, the brain will adapt to it’s surroundings and push us to danger.)
Now in itself, emotions are generated in our limbic system, used in a lot of adolescents as explained before. Each emotion is made from a different ‘network’ of brain modules, particularly the hypothalamus and pituitary gland, which control the hormones that produce physical reactions such as severely increased heart rate or even muscle contractions.
When we are as young as a baby, child, teenager or even as a young adult, our brain is over sensitive to external factors that stimulate us and environmental factors and influences. This means that if someone people in these age groups are close to (such as a friend or parent) demonstrates certain behaviours, it’s quite likely for the child to copy those behaviors and characteristics. This is mainly due to the fact that the brain goes under its main structural and functional development during these ages, specifically in the prefrontal cortex, which is responsible for decision making, emotional regulation and impulse control. Neuroscientific research has shown that brain development actually occurs slightly past the age of 21, and fully stops at around the ages of 24 to 26. This makes adolescents and young adults particularly vulnerable to both positive and negative influences. As a result of this, exposure to substances like nicotine or other dopamine feeding drugs, specific environments or experiences (such as sexual or abusive trauma) usually leads to long term emotional and behavioral consequences (such as acting out, emotional dis regulation).
One of the most recognized factors that endangers the young brain is the use of substances such as nicotine or alcohol (this is due to the fact that nicotine exposure during the teenage years commonly leads to neural circuit formation, impair attention and a very likely chance of addiction later in life, commonly through vapes or nicotine pouches. On the other hand, alcohol consumption, even in minor amounts, has been linked to reduction of hippocampal volume, which affects memory and learning, which can even lead to temporary memory loss. The reason these substances affect the teenage and young adult in particular is due to the fact that their brain is also going through synaptic pruning and myelination, interference from these substances in particular can impair function and increase risk taking behavior a significant amount. Yet even with teenagers not taking any of these substances, they can still be affected through abuse and trauma, especially within their own homes. Special studies that have been conducted have shown that repeated exposure to emotional, physical and psychological abuse can result in “toxic stress”, a state where the body’s stress system is activated for prolonged periods. This can lead to high cortisol levels, which when sustained over time can damage important brain structures such as the amygdala, hippocampus and prefrontal cortex.
These changes can negatively affect emotional regulation and memories, and the ability to cope with even minor challenges. An example of this (in the home environment) would be when parents practice actions such as repetitive harsh disciplining, emotional unavailability or pure neglect which can significantly impact a child’s mental development. The essential aspects of good parenting which will have a positive remaining influence in a child would be constant emotional stability and resilience. In contrast to this, children who experience abuse are much more likely to face delays in cognitive development, difficulties in regulating emotions and an increased risk of mental health disorders such as depression, anxiety and stress. Other research also indicates that these types of individuals often struggle academically and socially later in life. This also applies to school, as even though they were intended to be safe spaces for learning, can also become sources of trauma, such as bullying (verbal, social or physical bullying) have shown serious effects both neurological and psychological. Victims of bullying consistently show experienced fear responses, signs of chronic anxiety and difficulty concentrating on long tasks. Additionally excessively punishments from teachers or unsafe environments create a lot of stress and fear, limiting engagement and a student’s academic performance. Adding on to this, research on childhood experiences highlights that early mild trauma can have long term impacts. Individuals with higher exposure are at a significantly higher risk of developing substance abuse issues, developing mental health and even physical health problems much later in life.
In conclusion, the developing brain is much more impressionable and influential by both environmental and social factors, and while substances shows clear risks just like trauma does, understanding these factors is essential in order to protect and support healthy brain development.
The main reason that the cardiovascular system exists is to pump blood around the body through the heart. Blood is the primary substance in every nook and cranny of our body, flowing through us constantly, and blood helps with several functions such as controlling cardiac output and vascular resistance. In cardiology, bloodletting, transfusion and circulation show exactly how much medicine has evolved recently, seeing as just a few centuries ago blood transfusion was only a theory.
To start if off, circulation is defined by the movement o blood through a closed loop system driven by cardiac output which is the result of heart rare and stroke value. Precise circulation doesn’t actually rely that much on cardiac output as it does on systemic vascular resistance (resistance that the left ventricle of the heart must overcome to eject blood into systemic circulation) and the oxygen content of the blood. The modern understanding of the circulatory system is more or less enhanced by the work of William Harvey in the seventeenth century. He proposed that circulation works in a dual cycle, where the blood is driven around the body in a circular motion and passes through the heart twice. Another major aspect in circulation would be the importance of efficient oxygen delivery, which is the cardiac output and arterial oxygen content, which itself is also dependent on hemoglobin circulation. Even with preserved cardiac function, a low amount of hemoglobin can significantly impair tissue oxygenation.
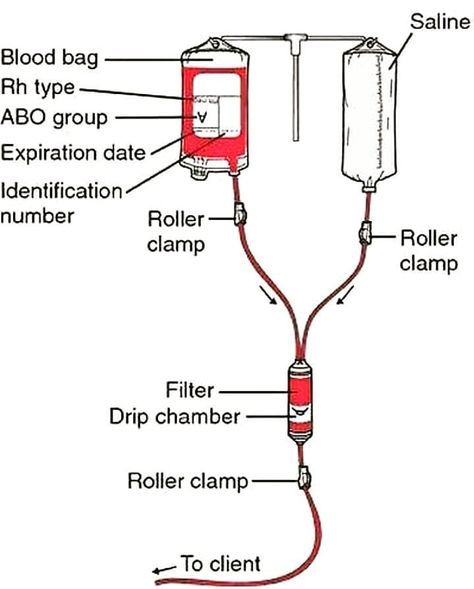
On the other hand, blood transfusion is used to replication oxygen carrying capacity and intro vascular volume, especially in patients that suffered from acute blood loss. In cardiology, this is especially relevant, particularly in acute coronary syndromes or decompensated heart failure. Doctors who actually perform blood transfusion usually prefer a more restrictive approach. In stable patients, transfusion is only considered when the patients hemoglobins level decrease lower than 7 g/dL. The main goal is to improve oxygen delivery and prevent potential adverse effects.
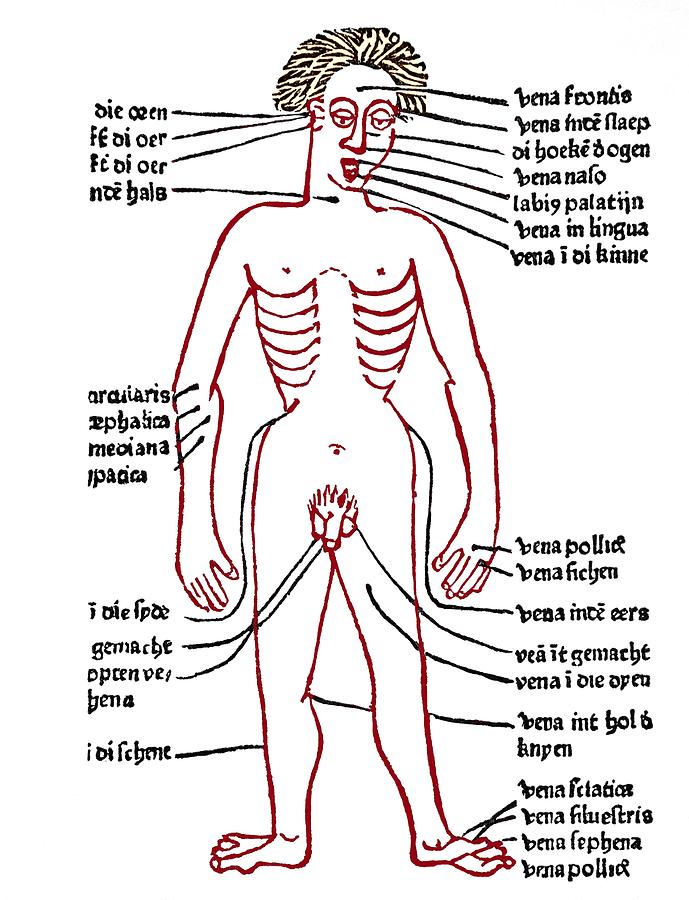
Now last but not least, bloodletting was first based on homunal theory and was before widely used across nearly every medical condition, while now it’s generally not a common treatment, and it’s more recent counterpart (therapeutic phlebotomy) remains quite relevant, particularly in hematologic disorders. In certain specific conditions such as “polycythemia Vera” and “hemochromarasis”, phlebotomy actually removes iron burden and blood viscosity. From a cardiovascular perspective, the lowering of a hematocrit helps improve micro vascular flow and reduce the risk of thrombosis as a whole, supporting circulatory efficiency. Phlebotomy is the perfect example of how older practices can be reintergrated to more modern treatments and used more effectively.
In conclusion, blood circulation, transfusion and removal are some of the most dire and necessary aspects of cardiology and cardiovascular management in general. They defined how we treat cardiology as a speciality and is the building blocks of the whole system.
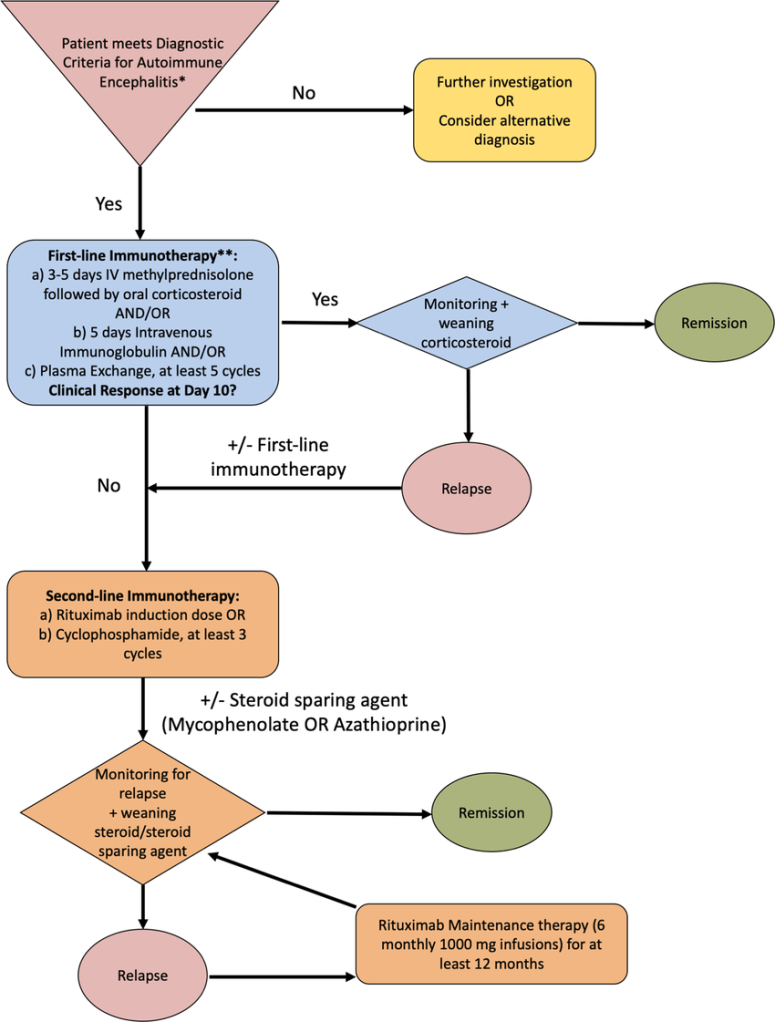
Pediatric autoimmune encephalitis was always interesting to me from the day I heard about it. When I read about it in the acclaimed Sunflower pediatrics book, I was confused. Adding to the fact that it was quite a rare disorder, I was bedazzled how the brain can be suddenly attacked by the immune system, leading to a whole load of neurological symptoms (such as memory loss, repeated seizures and not to mention inflammation!). When I learned there was a Google Meet organized discussing this topic and it’s causes, I evidently signed up.
Unlike the previous time, I was aware of this event quite a bit in advance, so I joined right in the nick of time, and saw several famous doctors that I have examined before in numerous pamphlets and medical papers. After some brief introductions, the board announced that over 300 people all over the world were attending this meeting, and I was absolutely flabbergasted by the amount of people, likely very similar to me. After recovering from that fact, the meeting went on.
Several doctors presented their case studies before we delved into the sub topics, but one case study really stood out to me over anything else. Before I present it, I have to state that pediatric autoimmune encephalitis is not a direct genetic disorder, meaning that a child can contract the disorder out of nowhere. While a family history of other autoimmune diseases can increase the likelihood, most patients have near no genetic history of these kind of diseases. As I was stating, the case study was of a young girl, aged around 9 years old, who suddenly contracted the disease, and with no family history surrounding her, the doctors weren’t able to diagnose where the disorder originated from. Luckily, a few days after she was in the hospital, they found out it was due to an exposure of the bacteria streptococcus, which can be found on skin and on animals.
The part that really interested me in this case was it showed how deadly the disease actually is, as it starts of with brain inflammation symptoms, which can by itself kill you, but with so much more symptoms it is quite terrifying, predominantly such as impaired thinking, numbness, seizures and loss of consciousness (even leading to prolonged comas).
Once we later moved on from the case studies, we delved right into treatment, ranging from antibody testing to therapeutic treatment, which really intrigued me due to the fact that it has proven to be very effective in these sort of cases, which is really heartwarming to me. Overall, it was just as fun as the previous meeting, and I’d love to delve in more.
During the summer, I got much more into medicine. I completed numerous courses on various academy websites, and constantly emailed many doctors about all the questions I had. Eventually, around a term break after school had started, I had got invited to attend a conference at a hospital with Dr. Hadi and Dr. Pawan as panelists and speakers. I was so nervous and worried, and revised multiple notes and blog posts and literally everything that had to do with neurology. I constantly emailed Dr. Hadi, asking a lot about the conference, and about nearly every single question about medicine that popped up in my head. Unfortunately, I never attended the conference, as I wasn’t able to obtain passes. As sad as I was, I got a phenomenal opportunity the next day, at around 5:30 p.m! Apparently, Dr. Hadi was hosting an online meeting, with around 2 other speakers and 2 panelists, each legends in the field of neuroscience!
At around 5:55, I was hurrying around my living room, scouring inch and inch for my notebooks, pens, headphones and electronics, and screaming the whole house down finding them, and finally, at around 5:58, I managed to join the call, out of breath, thankful for the fact that audio and video were disabled, but that didn’t hinder my enjoyment from the meeting. When it finally started at precisely 6, the chat comments were flooded with doctors and people like me (but older) registering and giving their details, and it honestly astonished me around how many people have the same interests and curiosity as me, and it just showed me as how minimal knowledge I have compared to people around the world, from the United Kingdom to Mexico!
The call started with a brief introduction to a lot of the doctors and panelists, and it really showed me just the amount of work and dedication these people put into their craft and work, and just how much of a passion they have for this, and it’s such an inspiration.
What really pleased me about this conference was that it wasn’t a robotic lecture about certain parts of neuroscience, but an interesting, pull-you-in conference, where the doctors displayed numerous case studies and examples, showcasing their own work and what they have done, and the diagnoses they have given based on the patient. It ranged from conditions of children who had infantile, epileptic spasms, (which consists of jerky movements and usual development regression, where the child is very behind his developmental milestones), and how they were able to diagnose his condition based on his numerous symptoms, to conditions where the child was a teenager and tragically died due to an unhealthy amount of ingested alcohol (at the age of 14).
It started off with the case study of a child with mild weakness in his body, where he could walk but was unable to balance, with a decline in his movement skills. He was overall behind in his physical and mental skills, with inability to perform his daily tasks without getting slurred and tired. After numerous gait tests and neurological examinations, they diagnosed the child with MLD, and the child moved abroad for further examination. MLD is the condition which affects a bodies white matter, and is actually relatively uncommon, found in ~ 1 in 40,000 people. The treatment method they used to treat him for the time they had (and the treatment evidently used in the country the child had travelled to) was Gene Therapy with Atidarsagene Automecel, which uses other functional genes to create genetically modified cells, to summarize it.
They showed other case studies and their treatment, and also accompanied with tips. The most important tip I personally took from the meeting was related to forgetfulness. Many doctors and neurologists tend to focus on what’s currently going on, and not other possibilities, no matter how unlikely. This can lead to other treatments not being used, which in the long term can be deadly to the patient. A core example is the one I mentioned previously, the teenager drinking and dying. This could’ve been prevented by checking ammonia levels, but nobody had thought to check that, leading to the sad death.
Overall, the meeting introduced me to numerous more topics and showed me so much more examples of conditions and symptoms than I thought possible before, and the significant amount of treatment plans that exists. It was so fun, listening to so much doctors give their own opinions and critical overviews on all the topics, and the sheer amount of questions I (and numerous [I mean numerous!] amount of people) asked. It was such a fun meeting, and I would love to attend another one soon!
Before I went to the Epilepsy Awareness event, I had a minimal knowledge of it. All I know was that when children diagnosed with this were prone to seizures and sensitive to certain events such as loud noises or intense physical pain. After this event though, I have gained such a more understanding of this topic, reading neurosurgery research and brain books, gaining a much greater insight into epilepsy and neuroscience as a whole. What I am here to discuss is my research that covers Epilepsy treatments and how Neurosurgery can help with these treatments and epilepsy as a whole.
Causes of Epilepsy should, foremost, be discussed first. In general, epilepsy, or seizures, are classified as sudden electric shock-bursts in the brain, leading to these patients having seizures or fits, where patients can suddenly not respond to anything, and certain physical traits are noticeable, such as eyes convulsing or arms and legs shaking vigorously. Though not all seizures are quite dramatic, as some patients can just stare blankly or slightly twitch. Many people can see these as just normal behaviors, so when these patients inform others, people do not usually believe them, which reminds me of how genuinely misunderstood and isolating this condition is. Epilepsy can also be caused due to other factors, like genetic disorders, infections like meningitis and brain malformations. Seizures can either be on one part of the brain, focal, or on both sides, generalized. Medication can help reduce seizures as a whole, though people who take medication can have balance/speech issues, evident that epilepsy can affect long-term development.
The second topic of this paper is treatments to epilepsy.
Medication; Usually anti-epileptic drugs (AEDs) such as Sodium valproate, carbamazepine, levetiracetam. They usually help reduce seizures but can cause side effects such as noticeable tiredness or unusual mood changes.
Surgery; this is for children whose seizures don’t respond to medicine, surgery is usually the second option. The most common form of neurosurgery for this is a “hemispherectomy”, where they disconnect and remove one brain hemisphere. This sounds quite extreme and fatal, but this neuroplasticity allows the brain to adapt, especially with early rehab.
Therapy; while this isn’t essentially a ‘treatment method’, this evidently helps the patients mentally and physically. The three most prominent forms of physiotherapy used to heal an epileptic patient are “Physiotherapy; helps with movement and muscle strength”, “diet therapists, people who help with diets, such as keto (this diet with high fat is shown to reduce seizures in certain patients),” and “occupational therapy, which supports daily functioning”
Neurosurgery also plays an important role in managing severe/drug-resistant epilepsy. When seizures start or originate from a certain area of the brain which can be able to be safely removed, such as a small legion or a scar, ‘focal resective surgery’ is permitted to be performed. In some more complex cases, where one hemisphere can cause all seizure activity, a functional disconnection may be vital, and these procedures are evidently more effective when done earlier, taking advantage of the brain’s plasticity, especially in children.
In conclusion, epilepsy affects more than just the brain, it shapes our daily life, education, emotions and our surroundings. With early diagnosis, medication and therapy, most people can live completely fulfilling lives. Seeing clinicians work closely with families reminded me that treatment is about people, not prescriptions. I think my time at the Epilepsy Awareness event really showed me that.